
Painful bladder conditions are common. Interstitial Cystitis (IC), otherwise known a Painful Bladder Syndrome, is one of the causes. People with IC suffer pain when the bladder is full and/or have to urinate frequently. The cause is unknown and diagnosis may take several visits to doctors and is predominately based around excluding other possible causes for the symptoms like and infection as there is no conclusive test to prove someone has interstitial cystitis. Diagnosis is based on clinical symptoms.
Nine out of ten sufferers are women. It can develop at any age, with the onset for most patients around the age of 40 years. Many women are diagnosed in their 30s.
IC is a chronic, debilitating syndrome and people respond variably to treatment. There is no cure, but patients may achieve long remissions.
What are the symptoms of Interstitial Cystitis?
- Pain. The main symptom is pain when the bladder is full, with a feeling of some relief on voiding, or emptying, the bladder. Pain may be felt in the pelvis, abdomen and in the vagina. Pain may be worse with bladder filling, voiding or during sexual intercourse. Men may feel pain in their prostate, scrotum or penis.
- Frequency. Having to urinate frequently, including overnight, is a classic sign of IC. People with the condition may urinate 40 or 50 times in 24 hours in most severe cases compared to the usual seven or eight.
- Urgency may also develop. This means a person is unable to delay urination and they may feel an urge to urinate even immediately after doing so. It is usually not associated with urinary leakage or a fear of leakage. Some describe a constant desire to pass urine.
What causes Interstitial Cystitis?
The cause of IC is unknown but several theories are being investigated.
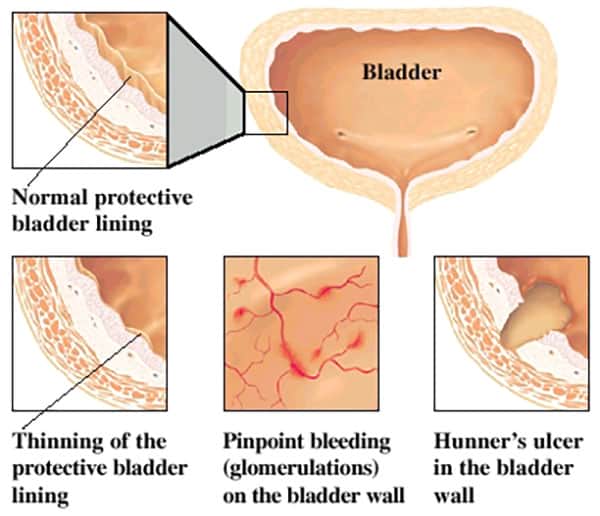
- Leaky bladder lining. IC might be caused by a defect in part of the inner lining of the bladder, the so-called glycosaminoglycans (GAG) layer. This could allow urine to irritate and inflame the bladder.
- Histamines. IC symptoms may be caused by an allergic reaction leading to the release of histamines from cells (known as mast cells) in the bladder wall. The histamines cause swelling and inflammation of the bladder lining.
- Autoimmune response. The body s immune system may attack the bladder. IC is more common in women with autoimmune conditions.
- Toxic urine. It may be that there is an agent in the urine of sufferers, which inflames the bladder.
- Post-surgical condition. IC is known to occur after hysterectomy but the reasons why are not clear.
- Anti-inflammatories. The use of non-steroidal anti-inflammatory drugs (NSAIDS) has been linked to IC, especially tiaprofenic acid (Surgam).
- Infection. IC might be caused by an as yet undiscovered trigger, such as a viral infection.
How is Interstitial Cystitis diagnosed?
No simple test diagnoses IC. Instead, a specialist will take a medical history from the patient, perform a physical examination, and suggest several investigations to rule out other conditions such as overactive bladder, endometriosis, infection, and cancer.
- A sample of urine will be tested to check for infection. Usually it is found to be normal in people with IC.
- The doctor might perform a cystoscopy: a telescope is introduced to the bladder through the urethra. Most of the time, the bladder lining looks normal, but, rarely, a red patch may be seen in the dome (Hunner’s ulcer), which is diagnostic of IC.
- Often the doctor will instill sterile water or saline into the bladder to distend it (hydro-distension). This can demonstrate multiple tiny spots of bleeding from the bladder lining when the fluid is released called glomerulations, which is highly suggestive of IC.
- A biopsy will be taken to exclude other diseases including malignancy.
How is Interstitial Cystitis treated?
A range of treatments may be tried before a patient achieves remission. These treatments are usually offered in a step-by-step process to see what works for each individual.
- Hydro-distension (filling the bladder with saline while under anaesthetic), which is undertaken as part of diagnosis, can also relieve symptoms in about half of patients. Weeks or even months of relief may follow, and the procedure can be repeated if successful.
- Oral drugs can also be helpful. These include:
- Amitriptyline, an antidepressant used to block pain. This drug has sedating and anti-cholinergic (suppression of urge to urinate) effects.
- Anti-histamines, believed to reduce inflammation in the bladder.
- Pentosan polysulfate (Elmiron), a drug specifically approved for IC which is designed to restore the GAG layer of the lining of the bladder wall to protect it from irritants in the urine which cause inflammation. This is not on the PBS and costs about $200 per month. Unfortunately it also does not work for many people. Side-effects include gastrointestinal upset and liver dysfunction.
- Gabapentin, a pain modifier.
- Bladder instillation. This involves a weekly visit to the doctor for about six weeks to receive drugs directly into the bladder via catheter (sometimes under anaesthetic). The substances used include:
- Dimethyl sulfoxide or DMSO (Rimso-50), a chemical solvent from wood pulp, which has several uses in medicine. It is known to reduce inflammation and block pain in about a third of IC patients. It is a potent destroyer of free radicals that damage cells. It has the rather bizarre side-effect of leaving patients smelling of garlic.
- Heparin, an anti-coagulant which is sometimes mixed with DMSO.
- Steroids mixed with DMSO.
- BCG, an agent used to stimulate the bladder’s immune system.
- Chlorpactin washout of the bladder under and anaesthetic.
- Surgery. When all else fails, and particularly when the patient has a progressive condition where they are losing bladder volume, surgery can be considered. Types of surgery:
- Sacral neuromodulation. Electrodes are implanted in the lower back, which block nerves that transmit pain from the bladder. This procedure should be carried out in specialist centres.
- Urinary diversion (ileal conduit). This operation allows urine to by-pass the bladder and be collected in a bag on the outside of the abdominal wall. Despite the body image issues created by this option, many patients value the freedom it gives them because they do not have to worry about proximity to a toilet. Over time some people who have had this operation may suffer deterioration of their kidneys.
- Bladder reconstruction. Part or the entire bladder is removed and then reconstructed from a segment of the bowel. This expands the capacity of the bladder but pain may persist.
- Bladder removal (cystectomy). Very occasionally, when pain persists despite urinary diversion, the bladder may be removed. Even still pain can persist.
What else can a patient do?
- Seek support. Patients living with interstitial cystitis can derive comfort and empowerment, as well as a lot of useful information, through their contact with others suffering the condition. Visit the Interstitial Cystitis Support Group of Australia website for more information or contact by writing to P.O. Box 767, Kingswood, NSW 2747.
- Modify diet. Some foods and drinks are known to make symptoms worse in many patients. These include tomatoes, citrus fruits, bananas, chocolate, cheese, mayonnaise, nuts, onions, raisins, sour cream, yoghurt, spicy foods, coffee, wine, beer and carbonated drinks. Patient support groups are often a good source of information about bothersome foods. Not everyone will be affected the same way so many people try an elimination diet, cutting out suspect foods one by one to see which may cause symptoms.
- Attend to mental health. Living with interstitial cystitis can cause significant stress and psychological effects. Constant sleep deprivation because you have to get up and go to the toilet impacts severely on a patient’s well being. Patients may feel tied to the toilet and unable to have a normal life, which also affects their mental health. The stigma associated with this kind of condition, coupled with chronic pain, can wear people down. Anti-depressants prescribed as a pain moderator may also help improve a patient s psychological state. Joining a support group (see above) can help too.
What is the prognosis for patients?
Most commonly, patients will have symptoms grumbling on and off for years. They will undergo a treatment, achieve remission, then find that symptoms return and may have to try something else. Interstitial cystitis is a condition, which tends to recur.
A smaller group of patients will progressively lose bladder volume. Despite treatments progressive scarring of the bladder wall occurs, so not only does pain persist, but bladder volume reduces. These patients are often candidates for urinary diversion surgery.
A third group of patients appears to fulfil the diagnostic criteria for interstitial cystitis at first but recovers completely. Urologists believe that if the condition becomes cured it probably was not interstitial cystitis in the first place.
Where can I get more information?
The following websites may be of interest:
The American Academy of Family Physicians' site for patients
Urology Channel patient information
International Painful Bladder Foundation
Interstitial Cystitis Association
Your urologist can help you to understand this condition, and work with you to determine the best treatment for you.