
Why do I need an Artificial Urethral Sphincter (AUS)?
You leak urine uncontrollably due to a weak sphincter muscle. In men this can occur occasionally after prostate surgery. If incontinence is severe and does not improve over time with pelvic floor exercises I may recommend insertion of an artificial urinary sphincter.
What is an AUS?
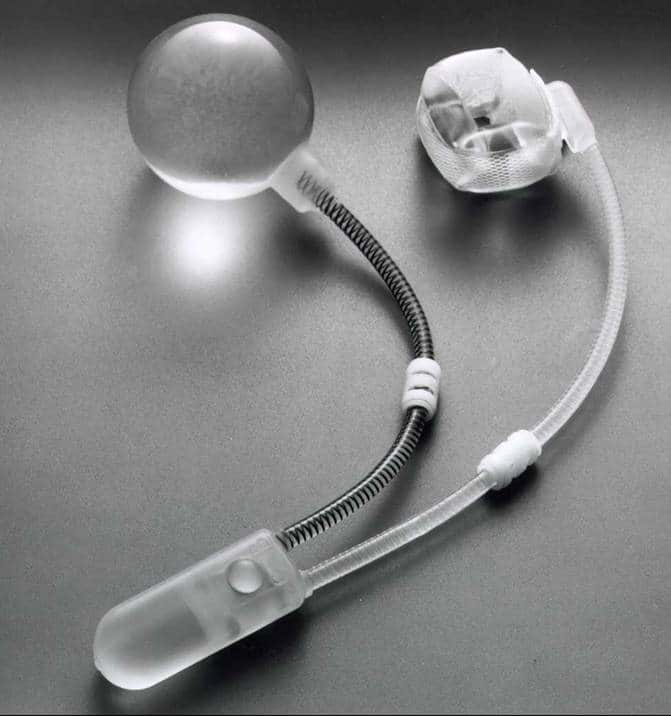
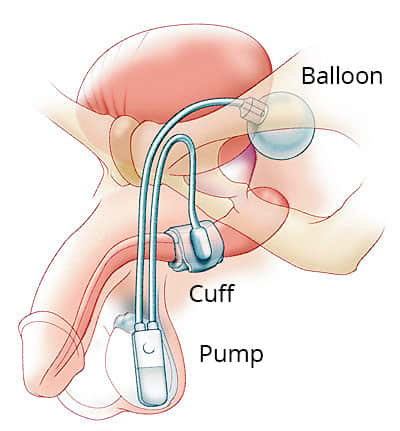
An AUS (Artificial Urinary Sphincter, or Artificial Urethral Sphincter) is a mechanical device inserted surgically in your body (as shown in the diagram), which takes the place of a poorly functioning sphincter muscle to help improve incontinence.
The device consists of a cuff, a pump and a pressure-regulating balloon. The cuff is placed around the urethra (water passage) and fills with fluid under pressure from the balloon reservoir, thus compressing the urethra and preventing urine from leaking out.
The pump is the part the patient squeezes to deflate the cuff when the bladder needs emptying. The pump is put under the skin where the patient can easily get at it (e.g. in the scrotum for men).
The pressure-regulating balloon is placed in the lower abdomen and is filled with fluid. After you deflate the cuff by squeezing the pump, the balloon will automatically refill the cuff after a minute or so, closing off the urethra once more. These three components are connected by plastic tubes, all under the skin.
How successful is the Artificial Urethral Sphincter operation?
There is a 90% success rate (where patients regain control of their bladder) from this type of surgery. 10% of patients will have some degree of ongoing bothersome urinary leakage.
Are there any alternatives to an Artificial Urethral Sphincter?
If you are not keen to have surgery, we can try convenes/sheaths or incontinence pads to manage your symptoms. Sometimes, a Male Sling (e.g. AdVance sling) device can be used for milder cases of incontinence in men.
Before your surgery
Please tell your surgeon (before your surgery) if you have any of the following:
- An artificial heart valve.
- A coronary artery stent.
- A heart pacemaker or defibrillator.
- An artificial joint.
- An artificial blood-vessel graft.
- A neurosurgical shunt.
- Any other implanted foreign body.
- A regular prescription for warfarin, aspirin or clopidogrel (Plavix®).
- Previous infection with an antibiotic resistant organism such as MRSA, VRE, etc.
What happens during the procedure?
Usually, you will be given a general anaesthetic (i.e. you will be asleep throughout the procedure). You will be given some antibiotics to reduce the risk of an infection.
You will have a small incision in the area between the scrotum and anus (the perineum) and the cuff will be placed around the waterpipe (urethra). A separate incision will be made in the lower abdomen or groin. Through this second wound, the pump will be placed in the scrotum and the balloon placed in the abdomen. A temporary catheter will be inserted during the operation, which will be removed before you are discharged.
In some cases, it may be possible to insert all the components of the sphincter through a single incision in your scrotum.
What happens immediately after the procedure?
You will usually be discharged 1-2 days after your surgery once the catheter placed during surgery is removed.
The artificial sphincter is kept deactivated (switched off) for 4-6 weeks after the operation to allow the body heal from surgery. There will probably be no change in your incontinence until the device is activated (switched on), and you should use pads or a sheath to control the leakage. Do not attempt to activate the sphincter yourself during this period. You will be reviewed in my rooms 4-6 weeks after the operation, when the sphincter will be activated. At this time, I will instruct you on how to use the sphincter.
Are there any side effects?
Most procedures are straightforward; however as with any surgical procedure there is a chance of side effects or complications.
Common (greater than 1 in 10)
- Blood in the urine, and temporary stinging when you urinate after the procedure.
- In the long-term, mechanical failure of the device (most devices will last over 10 years).
Occasional (between 1 in 10 and 1 in 50)
- Urine infection.
- Wound infection.
- Temporary insertion of a bladder catheter.
- Later failure of the device as the cuff becomes lose around the waterpipe (urethral atrophy).
Rare (less than 1 in 50)
Erosion of the cuff through the waterpipe (urethra).
What should I expect when I get home?
You should take things easy, especially for the first 2 weeks. Heavy lifting or exertion may cause bruising and swelling and slow your recovery. After two weeks, you can resume most normal activities, but strenuous exertion including sexual intercourse is not advised until 6 weeks after your surgery.
Cycling, horse-riding and other activities that cause extra pressure on the perineal wound (between the anus and scrotum) should be avoided.
You may be given a short course of antibiotics to prevent infection.
Simple painkillers will also be provided, and laxatives should be used if you are constipated.
You can shower after 48 hours. It is important to keep your wounds clean and dry. You should wash daily and pat the wounds dry with a clean towel afterwards. Do not take a bath or swim for 4 weeks after your surgery.
Reasons to call your GP / Urologist
- The incision(s) become red, swollen, opens, or there is pus-like drainage.
- The skin around your incision(s) feels warmer than elsewhere.
- There is an abnormal odour or cloudiness to your urine.
- You have nausea and vomiting.
- You cannot move your bowels.
- You have chills or temperature greater than 38° C.
- You experience severe pain that is not relieved by pain medication.
Disclaimer
This information is intended as a general educational guide and may not apply to your situation. You must not rely on this information as an alternative to consultation with your urologist or other health professional.
Not all potential complications are listed, and you must talk to your urologist about the complications specific to your situation.